Hearing loss accounts for nearly 8% of dementia cases worldwide (roughly 800,000 cases per year). Scientists and medical professionals have found a strong link between hearing loss and dementia.
Researchers at Johns Hopkins University (JHU), located in Baltimore, MD, have studied associations between hearing loss and dementia for many years. A 12-year-long study including around 600 adults, led by Dr. Frank Lin, found that mild, moderate, and severe hearing impairment were risk factors for dementia and that as hearing loss worsened the individual was more likely to develop dementia.
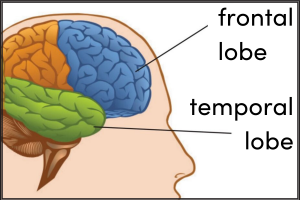
JHU researchers have used brain scans to show that hearing loss may contribute to a faster rate of atrophy (wasting away of tissue) in the frontal lobe and temporal lobe of the brain. These parts of the brain help with word production and understanding, problem-solving, planning, and emotion. Atrophy occurs because hearing loss puts a strain on the brain to work harder to hear. The brain working harder to hear comes at the expense of brain deterioration, which leads to thinking and memory deficits.
JHU researchers predict that the treatment of hearing loss with the utilization of hearing aids will reduce the stress placed on the brain to hear and minimize the risk of developing dementia. They have enrolled over 900 older adults who are participating in a clinical research study funded by the National Institute on Aging. The ACHIEVE study has finished recruiting participants and should complete collecting data within the next year. Study results should be published soon after.
Medical experts from JHU report that many wait too long to seek medical attention for hearing loss, as minor deficits in hearing can go unnoticed for some time. Research shows that even mild hearing loss can increase the risk of dementia. Seeking medical attention to combat hearing loss early can potentially reduce the risk of developing dementia. If you or someone you know is experiencing even mild hearing loss, refer to a primary care physician or an audiologist to see what treatment options are available for you to improve your hearing and potentially reduce your risk of dementia.
APOE is a gene that provides instruction for the body to make a protein called apolipoprotein E. Everyone has the APOE gene because we all need this protein which combines with lipids (fats) to carry cholesterol and fat-soluble vitamins through the bloodstream. The protein helps transport cholesterol to areas where it’s needed and out of areas it isn’t needed. Cholesterol helps the body build cells, and make hormones and vitamin D. This is important because it supports and repairs the central nervous system.
Genes can have different forms; these are called alleles. For example, genes related to eye color have more than one allele such as brown, blue, green, etc. Parents pass on genes to their children, but siblings may have different eye colors because one received an allele for blue eyes while the other received an allele for brown eyes. Scientists have discovered that APOE is polymorphic, meaning it has more than one allele (form). APOE has three major alleles: APOE-ε2, APOE-ε3, and APOE-ε4. Each person has two copies of the APOE gene, one from each parent.
In conversations about Alzheimer’s disease risk, APOE is often thrown into the mix, but why? In 1993, Dr. Judes Poirier led a study that helped push the topic of APOE into conversations about Alzheimer’s disease. Dr. Poirier led his team to research how the combination of alleles for the APOE gene may influence a person’s risk for Alzheimer’s disease. The research team used blood tests from 91 Alzheimer’s patients and 74 people without Alzheimer’s to determine their alleles for the APOE gene. Results showed that Alzheimer’s patients often had a copy of the APOE-ε4 allele. This allele did not show up as often in the individuals without Alzheimer’s. This led to the conclusion that when a person has an APOE-ε4 allele they may be at a higher risk for Alzheimer’s disease than someone without an APOE-ε4 allele.
Continued research since 1993 shows APOE does not tell the whole story about Alzheimer’s disease. It is certainly associated with risk for the disease. But it does not determine if a person will develop Alzheimer’s because not everyone with an APOE-ε4 allele is diagnosed with the disease. Scientists are continuing to explore genetic-related questions about Alzheimer’s to increase their understanding of the involvement of genes.
Genetic research in relation to Alzheimer’s disease became a topic of conversation in 1993 when Dr. Judes Poirier led a research team to study how the APOE gene may influence a person’s risk for Alzheimer’s disease. The published journal article that shared the results from this study is the first one on our list of 5 Research Articles About APOE. Since 1993, scientists have continued genetic-related research studies to explore this topic. The articles on our list span the past 20 years. They are listed in chronological order, with Dr. Poirer’s 1993 article as the first and an article from 2022 as the last.
Numerous research articles have been published on APOE and Alzheimer’s disease. Here are five genetic research studies on this topic that we found interesting:
1. APOE in 1993
Apolipoprotein E Polymorphism and Alzheimer’s Disease, written by Dr. Judes Poirier and colleagues, was published in 1993.
The study was completed with 91 people diagnosed with Alzheimer’s and 74 people without Alzheimer’s. Blood samples were used to determine their specific alleles for the APOE gene. Results showed that Alzheimer’s patients often had a copy of the APOE-ε4 allele. This led to the conclusion that when a person has an APOE-ε4 allele they may be at a higher risk for Alzheimer’s disease than someone with an APOE-ε2 or APOE-ε3 allele.
2. APOE and Cognitive Decline in Active Professional Football Players
Lower Cognitive Performance of Older Football Players Possessing Apolipoprotein E ε4, written by Dr. Kenneth Kutner and colleagues, was published in 2000.
As the title suggests, the research team was trying to find the relationship between APOE alleles and cognitive decline in football players. There were 53 active American professional football players who participated in the study by providing a saliva sample and doing cognitive assessments. 14 of the players had one copy of the APOE-ε4 allele. Players were both younger with low exposure to contact (head injury; concussion) and older with high exposure to contact. Results showed that APOE-ε4 carriers with high exposure scored lower on the cognitive assessments than the other participants. The authors gather that APOE status may affect the ability of the brain to heal after a football contact-related injury. Further research is needed to explore this idea.
3. APOE Alleles
Apolipoprotein E and Alzheimer Disease: Risk, Mechanisms and Therapy, written by Dr. Liu Chia-Chen and colleagues, was published in 2013.
This article takes a deeper dive into how an APOE protein will act in the body, depending on the alleles responsible for creating it. The most common alleles of the APOE gene are ε2, ε3, and ε4. The authors review current information known about the way various combinations of these alleles affect the central nervous system. This information is then linked to Alzheimer’s disease and other dementias to give a clearer picture of how APOE affects risk for these diseases through the impact on the protein it is responsible for creating.
4. APOE and Diet
Genotype Patterns at CLU, CR1, PICALM and APOE, Cognition and Mediterranean Diet: The PREDIMED-NAVARRA Trial, written by Dr. Elena Martinez-Lapiscina, was published in 2014.
This research group explored the relationship between diet and cognitive decline. A total of 522 participants were enrolled in the PREDIMED-NAVARRA study, and they followed a traditional Mediterranean diet (MedDiet) or a low-fat diet. The MedDiet consists of olive oil as the main fat, lots of plant-based foods, moderate amounts of fish and dairy products, and low amounts of meat. The authors were interested in the diet’s ability to improve cognition and if a person’s genes would have an impact. Due to the low number of APOE-ε4 carriers in the study, the authors couldn’t determine if the gene impacted the effects of diet on cognition. However, this article also explores genes other than APOE. CLU, CR1, and PICALM genotypes were also studied. This allowed the research team to look at individual gene influence and genetic profile (combination of various forms of genes) impact.
For example, results showed that after following the MedDiet, participants with at least one copy of the CLU-rs11136000 gene variant, also known as the T allele, improved their scores on a cognitive assessment that examined orientation, verbal recall, language, and visual construction.
Similarly, results showed that after following the MedDiet, participants with a genetic profile consisting of the CR1-rs3818361, CLU-rs11136000, and PICALM- rs3851179 genes, significantly improved their scores on a cognitive assessment that observed executive function and visuospatial skills.
5. APOE and Obesity
5. Reduced Brain Activity During a Working Memory Task in Middle-Aged Apolipoprotein E ε4 Carriers with Overweight/Obesity, written by Dr. Jermon Drake and colleagues, was published in 2022.
This article summarizes a study of 48 adults who completed a working memory task during an MRI scan. A working memory task is a type of cognitive assessment that measures short-term memory. For example, this study used a task setup to ask participants if the letter presented on the screen is the same as the letter shown before that letter or the letter before that. This research study observed how the brain activates during the task. Results concluded that obesity and the APOE-ε4 allele are both risk factors for cognitive decline.
What Will be Published Next?
Researchers continue to explore interventions and therapies that might be more beneficial for individuals with a genetic risk for Alzheimer’s disease. For example, the Physical Activity and Alzheimer’s Disease 2 (PAAD2) study, led by Dr. Jenny Etnier, is underway and will be joining the body of literature found on the important topic of APOE and Alzheimer’s disease. If you want to learn more about how PAAD2 is contributing to answering questions about Alzheimer’s disease, click here.
What’s the Difference Between Dementia and Alzheimer’s Disease?
Posted on February 15, 2023
The terms Dementia and Alzheimer’s disease are often used interchangeably. They share many similarities such as symptoms of memory loss and disorientation. Both are caused by damage to nerve cells and their connections in the brain, which lead to changes in a person’s thoughts and behaviors. Nevertheless, they are two different medical terms.
Dementia is a general term for the decline of cognitive functioning severe enough to interfere with daily life. The symptoms and characteristics of an individual experiencing dementia may include memory loss, difficulty problem-solving, and/or confusion. There are different types of progressive dementias, meaning dementias that progress and are not reversible. The type of dementia someone may have is associated with how their brain is affected, such as vessel damage, protein clumps, or fibrous tangles.
Alzheimer’s disease is one of the types of dementia and it is the most common type. It accounts for 60-80% of all dementia cases. Alzheimer’s disease affects memory, thinking skills, and behavior. As the disease advances, it can lead to more severe symptoms such as disorientation, mood changes, confusion, suspicions, and motor behavior difficulties. Alzheimer’s disease patients have plaques and tangles in their brains. Scientists do not know exactly what these plaques and tangles do but expect they are damaging nerve cells and their connections in the brain.
Plaques are deposits of a protein fragment called beta-amyloid that build up in the spaces between nerve cells.
Tangles are twisted fibers of another protein called tau that build up inside nerve cells.
Dementia and Alzheimer’s disease also share common risk factors. There are a couple that cannot be changed, such as age and family history. However, there are several risk factors that you can change! Research shows a greater risk of dementia in people who eat an unhealthy diet, drink large amounts of alcohol, experience sleep disturbances, have hypertension, and experience air pollution exposure.
Start with something simple and small as a step toward reducing risk for Dementia and Alzheimer’s disease. Add a cup of fruit or vegetables to each meal. Change your air filters regularly. Attend yearly physicals and talk to your doctor about any concerns.
Dementia Associated With Resting Heart Rate: What the Research Says
Posted on February 21, 2023
What is Resting Heart Rate?
Your heart rate, or pulse, is the number of times your heart beats in 1 minute. Heart rates vary from person to person. It’s lower when you’re at rest and higher when you exercise. Resting heart rate (RHR) is the number of times your heart beats in 1 minute when you are at rest or relaxed, such as when you are sitting or lying down. According to the American Heart Association, a normal RHR is between 60 and 100 beats per minute (bmp) for adults.
How is Resting Heart Rate Measured?
RHR can be measured by doctors, researchers, and individuals. The Physical Activity and Alzheimer’s Disease (PAAD2) study collects RHR data during in-person assessments by placing electrode stickers on the research participant and using equipment to record the activity of the participant’s heartbeat. RHR can also be measured manually by an individual.
Steps to Check Your Own Resting Heart Rate
Sit down and rest for 5 minutes.
Turn your wrist so your palm is facing up.
Feel for a pulse at the thumb side of your wrist.
Once you feel it, count how many times you feel a beat in 30 seconds. Then double it.
If you have any concerns about your RHR, please see your doctor.
Is Resting Heart Rate Tied to Dementia?
Research has linked elevated RHR to cardiovascular diseases such as heart disease, atrial fibrillation, and stroke. These are also risk factors for dementia. Now, scientists have begun to explore the association between RHR and dementia. Two longitudinal studies, one in the United States and one in Sweden, utilized their data to investigate this association.
Study 1, Dr. Wang and Colleagues, The American Journal of Cardiology, 2019
The Atherosclerosis Risk in Communities (ARIC) study followed 13,720 adults, ages 44-66 when enrolled, for twenty years. RHR and cognitive scores were collected at baseline assessments from 1990-1992. Participants were healthy and showed no signs of cognitive decline. They completed cognitive assessments again around 1997 and 2012. Results showed that elevated RHR was associated with worsening cognition over time. Such that, participants with a RHR of 80 bpm or higher when they started the study were more likely to have a greater cognitive decline over 20 years and an increased risk of dementia compared with participants that had a lower RHR.
Study 2, Dr. Imahori and Colleagues, Alzheimer’s & Dementia, 2022
The Swedish National Study on Aging and Care in Kungsholmen (SNAC-K) followed 2,000 older adults from 2001 to 2016. Participants showed no signs of cognitive decline when they enrolled in the study and completed assessments of RHR and cognitive function every 3-6 years throughout the study. Results showed that elevated RHR was associated with dementia, such that older adults with a RHR of 80 bpm or higher had an increased risk of developing dementia compared with people whose RHR was 60-69 bpm.
It is important to note that the results from these studies show cognition is associated with RHR, not caused by RHR. This is where more research is needed. The results do confirm elevated RHR may be a sign of a health risk. Luckily, RHR is easy to measure and monitor, even from home. If you have any concerns about your RHR, please see your doctor. A reduction in RHR may be explored through diet, exercise, or medications.
Communication is an important part of life. It helps maintain relationships, build trust, and resolve conflict. A person with dementia needs to experience communication to preserve their self-worth and quality of life. However, talking and communicating with someone with dementia can become challenging.
The most common symptom of dementia is memory loss. Someone with dementia can be forgetful and sometimes struggle to find the right words to say. This can make conversations challenging. Talking and communicating can become even more tricky if they are experiencing other symptoms of dementia such as confusion, mood swings, or agitation.
According to the National Insitute on Aging (NIA), effective communication can help build satisfying relationships. Nevertheless, communicating is difficult for someone with dementia because they have trouble remembering things. Fortunately, there are ways to help make communication easier. Here are some tips for communicating with someone with dementia.
Pay attention to your body language and use physical contact when appropriate.
Body language is shown through nonverbal signals such as facial expressions, tone of voice, body posture, and gestures. A smile and calm voice signals openness and positive emotions. Consider the gestures you may be using. For example, pointing or shaking your finger at someone implies negative feelings. You may find it helpful to limit gestures while speaking with someone with dementia.
Physical contact may be used as a sign of affection and can create feelings of security. If you notice the person with dementia is feeling sad or nervous, offer comfort by squeezing their hand or placing your hand lightly on their arm. Emotions can change quickly so make sure to approach physical touch with caution.
Avoid distractions and keep things simple.
Limit visual and audio distractions by turning off background noise such as the TV or radio. These things can make it difficult to hear and concentrate.
Use simple words when speaking and wait a few seconds for a response. Ask one question at a time to not overwhelm a person with dementia. If they struggle to respond, try communicating with more statements and fewer questions. For example, say ‘we are going for a walk’ instead of ‘would you like to go for a walk?’.
Visuals are a great way to help navigate a conversation. For example, show a peach and a banana to a person with dementia when asking which one they would like for a snack.
Enjoy your time together and take a moment to reminisce.
A person with dementia can remember events from many years ago and these memories are very precious to them. Talk or ask questions about these memories. Look at photos that trigger positive memories.
If a person with dementia remembers something incorrectly, don’t worry about correcting them. This may lead to confusion or agitation. Instead, turn the conversation to something else.
Finally, remember to be patient.
Someone with dementia may require a change to the way they would communicate before symptoms of dementia began. As symptoms progress, more communication challenges may be present and additional changes may be needed. If you are feeling frustrated, it is okay to take a break. Consider starting with some small changes, such as limiting background noise during conversations, to help maintain positive relationships and keep stress levels minimal.
Dementia is a broad term used to describe a range of conditions that affect the brain. It is not a specific disease, but an umbrella term for several diseases characterized by the loss of cognitive functioning. In the same way that basketball and football fall under the category of sports, diseases like Alzheimer’s disease and Lewy body dementia fall under the category of dementia.
What these diseases have in common is that they affect the function of the brain. People diagnosed with a type of dementia will have a range of symptoms that affect their thinking abilities. The most common symptoms include memory loss, changes in behavior, and a decline in the ability to live independently.
The intensity of these symptoms can vary from person to person, which means some patients will need more assistance than others. Additionally, most types of dementia are progressive which means symptoms may worsen over time and unfortunately there is still no cure for any type of dementia.
Although we don’t know everything about dementia, research has given us the ability to identify and treat many of these diseases. The most common forms of progressive dementia include Alzheimer’s disease, vascular dementia, frontotemporal dementia, and Lewy body dementia.
Alzheimer’s Disease
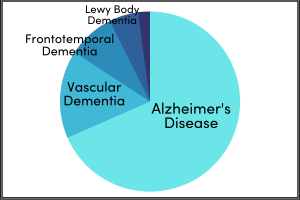
The most common form of dementia is Alzheimer’s disease (AD), representing 60%-80% of all dementia diagnoses. The cause of AD is unknown, however, people with AD are often found to have a buildup of clumped proteins in the brain, referred to as plaques and tangles. Common symptoms of AD include short-term memory loss, changes in behavior, and a decreased ability to carry out normal functions like getting dressed or driving a car.
Vascular Dementia
Accounting for 10-20% of all dementia diagnoses, vascular dementia (VD) is any dementia that is caused by damage to the brain’s blood vessels. Conditions that decrease blood circulation, like a stroke blocking an artery, may cause damage to the brain from impaired blood flow. Factors that increase a person’s risk of stroke and heart disease (diabetes, hypertension, high cholesterol, smoking, etc.) also increase the risk of VD. Common symptoms of VD include memory loss, slowed thinking, and loss of interest in things or people they previously enjoyed. It is common for people with VD to experience behavioral changes, such as irritability, that make them choose to be isolated.
Frontotemporal Dementia
Brain disorders that affect the frontal and temporal lobes of the brain are classified as frontotemporal dementia (FD). FD represents about 10% of dementia diagnoses and is caused by an abnormal protein forming inside the brain cells of the frontal and temporal lobes, causing the lobes to shrink. These lobes are important for processing information, including emotions. As a result, people with FD usually have distinct changes in behavior, personality, and language. They may say things that are rude and inappropriate, become impulsive, and in some cases, lose the ability to speak.
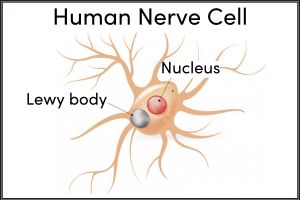
Lewy Body Dementia
Lewy body dementia (LBD) accounts for about 4% of dementia diagnoses. Lewy bodies are protein deposits that develop in the nerve cells in the brain; a person with this type of dementia has a buildup of Lewy bodies in the parts of the brain involved in thinking and movement. Common symptoms of LBD include memory loss, hallucinations, and problems with motor control abilities such as tremors and slow movement. Unfortunately, it is often common for people with LBD to become depressed and lose interest in things they once enjoyed.
According to the CDC, dementia diagnoses are expected to reach almost 14 million by 2060. This is why research studies, such as PAAD-2, are so important. Research about reducing the risk of dementia can provide life-changing information to potentially cut down the number of dementia diagnoses.
Recent Findings From the PAAD2 Study: Interview With The Author
Posted on April 25, 2023
MEET THE AUTHOR
Sam DuBois is a doctoral candidate in the Kinesiology department at the University of North Carolina at Greensboro. She has earned a master’s degree in Sport and Exercise Psychology and is currently working on her PhD. She has finished all coursework and is in the beginning stages of her dissertation. She plans to become a university faculty member to teach and pursue research.
Ms. DuBois’ faculty advisor is Dr. Jenny Etnier, Julia Taylor Morton Distinguished Professor, Kinesiology Department Chair, and Principal Investigator of the Physical Activity and Alzheimer’s Disease 2 (PAAD2) Study. The PAAD2 Study is a federally funded research project that explores the protective benefit of exercise for people with a family history of Alzheimer’s disease or dementia. Ms. DuBois has been a part of the PAAD2 research team as a graduate research assistant since 2019. She leads cognitive, exercise, and MRI assessments and is a level IV MRI operator. She also helps with processing data, scheduling assessments, and leading MRI training sessions for students.
Sam DuBois and Dr. Etnier at the UNCG Graduate Research Showcase
FORMING THE RESEARCH QUESTION
As an involved member of the PAAD2 research team, Ms. DuBois is hands-on with data collection (e.g., working with study participants, running the MRI equipment, etc.) and data analysis (e.g., inspecting data with statistical computer programs, interpreting results, etc.). She uses these experiences along with knowledge learned throughout her time as a graduate student to explore unanswered research questions. Recently, Ms. DuBois worked with Dr. Jenny Etnier, Dr. Shin Park, Dr. Chris Wahlheim, and Dr. Laurie Wideman as mentors and co-authors on her research titled, The Association Between Aerobic Fitness and Mnemonic Discrimination in Middle-Aged Adults at Genetic Risk for Alzheimer’s Disease. We were able to ask her some questions about this project to learn more.
Can you walk us through the title and what it means?
My research is exploring the question, does APOE ε4 carrier status influence the relationship between aerobic fitness and mnemonic discrimination? The data is from participants who are part of the ongoing PAAD2 study. They are all between the ages of 40 and 65 and have a family history of Alzheimer’s disease (AD) or dementia. Individuals who carry the Apolipoprotein E (APOE) ε4 allele are at a heightened genetic risk for AD. We used saliva samples to determine APOE ε4 carrier status (carriers or non-carriers). This information was used to examine if APOE ε4 carrier status and aerobic fitness predicted performance on a mnemonic discrimination task sensitive to hippocampal integrity.
Aerobic fitness was measured by walking on a treadmill with an assessment called a submaximal exercise test.
Mnemonic discrimination was measured by performance on a modified object recognition task.
How did you come up with this research question?
Existing research shows three key things related to forming this research question:
1. During the early stages of AD, the hippocampus experiences detrimental changes that impair its ability to form distinct memories (Rao et al., 2022). This is why memory problems for recent information are often the first noticeable symptom of the disease.
2. APOE ε4 carriers are at a heightened genetic risk for AD (Corder et al., 1993) and exhibit hippocampal changes even in the absence of AD symptoms (Lind et al., 2006).
3. There is a positive association between aerobic fitness and hippocampal integrity. Adults who have higher aerobic fitness also have greater hippocampal volume and better hippocampal function (Erickson et al., 2009).
However, it is unclear how a person’s genetic risk for AD influences this relationship between aerobic fitness and hippocampal integrity. Exploring this interaction could lead to preventative interventions aimed at preserving the integrity of the hippocampus and the memory abilities it supports for those at a heightened genetic risk of AD.
The term mnemonic discrimination is not used in everyday conversations, what is it?
Mnemonic [nuh-MON-ik] discrimination is the ability to differentiate a current event from similar past events. For example, to remember the location of your parked car, you must differentiate your current parking spot from all the parking spots you have previously occupied. Most days we can successfully do this, but other days we may stand in the parking lot frustrated and confused unable to remember the location of our parked car because of the interference created by existing memories for our previously occupied parking spots.
Our mnemonic discrimination ability is enabled by the hippocampus and its ability to form highly detailed, distinct memories (Yassa & Stark, 2011). Unfortunately, because mnemonic discrimination is dependent on the hippocampus, it is often one of the first memory abilities impaired by AD. Since APOE ε4 carriers are at a heightened genetic risk for AD and exhibit hippocampal changes even in the absence of AD symptoms, they are also at risk of experiencing declines in mnemonic discrimination.
In a research setting, we can examine a participant’s mnemonic discrimination with a specific type of memory test. The PAAD2 study uses the Mnemonic Similarity Task created by Dr. Stark and colleagues (Stark et al., 2019). During this task, participants first study images of everyday objects and decide if each object is an “indoor” or “outdoor” object. Then they complete a memory test during which they indicate if objects are the exact same as previously studied objects, similar but not identical to studied objects, or entirely new objects. The ability to differentiate “similar” objects from previously studied “old” objects reflects successful mnemonic discrimination and is sensitive to hippocampal integrity.
FINDINGS AND CONCLUSIONS
To examine the data, statistical computer programs are used. The information that is outputted is then interpreted into results. Ms. DuBois’ uses statistical devices such as graphs, p-values, and correlation coefficients when presenting results in poster and PowerPoint presentations. Then, the results provide meaningful information about the research question.
After looking at all this data, what were the findings?
After analyzing the data, I found that for the objects that are the most “similar” to previously studied objects and therefore the most difficult to discriminate between, there was a statistically significant interaction between APOE ε4 carrier status and aerobic fitness. This interaction indicates that higher aerobic fitness is associated with better mnemonic discrimination only for the APOE ε4 carriers. In contrast, for the APOE ε4 noncarriers no significant relationship was observed between aerobic fitness and mnemonic discrimination.
Since previous research has shown that APOE ε4 carriers are at a heightened genetic risk for AD and exhibit hippocampal changes even in the absence of AD symptoms, this finding suggests that having higher aerobic fitness may protect against some of these hippocampal changes that make these individuals more susceptible to experiencing impairments in mnemonic discrimination.
Why is this important?
These results suggest that aerobic fitness may benefit the hippocampal-dependent memory of those at a heightened genetic risk for AD. Developing physical activity programs aimed at improving aerobic fitness may therefore be a promising preventative intervention for this at-risk population.
SHARING THE FINDINGS
Ms. DuBois presented these findings at the UNCG Graduate Research and Creativity Showcase on April 4, 2023. This annual showcase presents the accomplishments of UNCG’s graduate students to the community. Graduate students explain and present their work through posters.
DuBois with her poster at the showcase
Graduate student posters displayed at the showcase
She also applied to present her work through a poster presentation at the North American Society for the Psychology of Sport and Physical Activity (NASPSPA) conference taking place this summer in Toronto. Not only was she accepted, but the reviewers asked Ms. DuBois to give a verbal presentation where she will speak to conference attendees about this research.
Music therapy has emerged as a promising intervention for individuals with Alzheimer’s disease. With its ability to stimulate memories and positive emotions, music has been shown to enhance cognitive and emotional functioning in those affected by the disease. As a result, music therapy has gained attention from scientists and research supports its ability to be used as a form of treatment for patients with Alzheimer’s disease and other forms of dementia.
Music therapy is a clinical intervention that uses music to address a wide range of physical, emotional, cognitive, and social needs. The goal of music therapy is to enhance overall well-being and improve quality of life. It can take many forms, depending on the individual needs and preferences of the patient. Some patients may enjoy listening to music, while others may prefer to sing or play an instrument.
For people with dementia, music can be a powerful tool for unlocking memories and improving communication. Listening to familiar songs from their past can help them to remember events, people, and emotions from earlier in their lives. Music can also stimulate conversation and encourage social interaction, which can be especially valuable for patients who have become socially isolated.
Furthermore, music therapy has been shown to have a positive impact on the physical and emotional well-being of patients with dementia. Music can reduce anxiety, depression, and agitation, which are common symptoms of dementia. Listening to music can also have a calming effect on patients, helping to lower their heart rate and blood pressure.
In conclusion, music therapy is a valuable tool for improving the quality of life for people with dementia. It can help to unlock memories, improve communication, and reduce symptoms of anxiety and depression. Scientists are continuing to study the potential benefits of music therapy to develop evidence-based interventions for patients with Alzheimer’s disease and other forms of dementia.
The IGROOVE Study at Wake Forest University in Winston-Salem, NC is exploring how music and dance may affect fitness and brain health for people concerned about their memory but who have not been diagnosed with memory loss.
The MELODY Study at the Medical University of South Carolina in Charleston, SC is working with Alzheimer’s patients to explore the impact of meaningful tunes by using MRI scans to identify how brain networks are modulated via exposure to this music.
The Virtual Music and Memory Study at the University of Southern California is an online study where researchers are working with older adults from underrepresented communities to learn how listening to music impacts memory processes. They are interested in music-evoked autobiographical memories which are strong personal memories, often with emotional content, which are prompted by a musical stimulus.
More than a hundred years ago, a German psychiatrist named Dr. Alois Alzheimer made an important discovery about a disease that would later bear his name. This discovery helped us learn more about the disease and laid the foundation for subsequent research and treatment.
The Mysterious Patient: In 1901, Dr. Alzheimer met a middle-aged woman named Frau Auguste Deter at the Frankfurt Asylum in Germany. She was not like other patients; she was suffering from symptoms that defied conventional medical explanations. She experienced severe memory loss, confusion, and behavioral changes. Dr. Alzheimer was curious about her condition and began observing and documenting her symptoms to better understand what was happening. This led to a big breakthrough.
Dr. Alzheimer’s handwritten medical file for Deter
Photo: Dr. Alzheimer’s handwritten medical file for Deter
The Final Examination That Showed the Truth: As time went on, the patient’s condition got worse, and she eventually passed away in 1906. Dr. Alzheimer looked at her brain during a post-mortem examination and uncovered distinct abnormalities. He found the presence of tangled nerve fibers and unusual protein deposits, now recognized as amyloid plaques and neurofibrillary tangles. These discoveries helped him understand more about what was happening inside her brain.
A New Disease is Named: Dr. Alzheimer’s discovery became the foundation for studying this disease. Scientists wanted to understand, diagnose, and treat this devastating disease. In 1910, a psychiatrist who worked with Dr. Alzheimer, Dr. Emil Kraepelin, named the disease “Alzheimer’s disease”. It was published for the first time in Germany in volume two of the book General Psychiatry.
Legacy and Ongoing Research: Dr. Alzheimer did not stop at his initial discovery. He wrote many papers about the brain and how it works. His research helped people understand more about Alzheimer’s disease. He laid the groundwork for future generations of scientists, who have built upon his findings, advancing our understanding of Alzheimer’s disease. For example, scientists have learned more about genes and created better machines to look at the brain. With these advances, doctors can detect the disease earlier and develop new treatments. Ongoing research, inspired by Dr. Alzheimer’s work, strives for effective treatments and prevention strategies, and ultimately, a cure.
Monument on Dr. Alzheimer’s former home, Villa of Wrocław
Image: Monument on Dr. Alzheimer’s former home, Villa of Wrocław
Dr. Alzheimer’s extraordinary discovery of Alzheimer’s disease has forever changed the medical world. His research helped us understand the disease better and find ways to help those affected. As scientists and healthcare professionals build upon his work, we continue to see new discoveries that improve the lives of those affected by Alzheimer’s disease.